
After writing a blog about placentophagy the challenge was to find a topic people wanted to hear about even less. Yesterday, I had my colonoscopy. Every now and then, it’s good for the physician to become the patient.
Colonoscopy was invented in 1969 by Drs. William Wolff and Hiromi Shinya and popularized as an advance over barium enema and flexible sigmoidoscopy. Colonoscopy allowed for visualization of the entire colon and for the removal of polyps.
Since polyps can take as long as 10-15 years to transform into cancer, colonoscopy has been recommended by most medical societies, including the American Cancer Society and the American Congress of Obstetricians and Gynecologists, as recommended health maintenance screening every 10 years, beginning at age 50, for both men and women at average risk for colon cancer.
Colonoscopy screening prevents approximately two thirds of deaths due to cancer on the left side of the colon. The evidence is less robust for a significant reduction in right sided colonic disease. Individuals at higher risk of colon cancer are recommended to have colonoscopies every 5 years. My mother beat colon cancer, but I’ve kept that a secret.
I had my first colonoscopy 12 years ago. The report said that nothing suspicious was seen. They hit me so hard with Versed that I have no memory of the entire day. I consider that a win-win. I skipped my 10 year anniversary colonoscopy. I thought it’d be weird to show up perfectly on time for another go.
My 11th year I cancelled because the University instituted a ridiculous plan to require pre-payment in full even if you had insurance coverage. That was accompanied by the lame promise to reimburse once insurance payment was received. First, I had a vague suspicion that was illegal. Second, I had personal knowledge of the relative sizes of the billing and reimbursement departments. The billing department is a city block with a thousand cubicles. The refund department reminds you a little of the lost luggage kiosk at the airport.
By my 12th year, the University had dropped that ill-conceived policy and I signed for colonoscopy number two. While I reveled in my victory over taxation without representation, I did worry how large my colon cancer had become while I was taking my moral stand. I wondered if karma was going to come back around and bite me in the butt – no pun intended.
Admittedly, I sometimes give the Medical University a hard time. However, let me say that everyone should come to MUSC for their colonoscopies. Hands down, slam dunk, not even close. I arrived on time at 11 am and valet parked at Ashley River Tower. Elevator D to the second floor reservation desk where I signed in. I was called back in less than 5 minutes. A nice nurse took a brief history, got my vitals and started an IV. I didn’t realize at the time, but the IV would be the worst part of the day.
I changed into my gown which was backless and I remembered why I was there. I started to obsess about the non-slip ankle socks. I can’t help it. I’m a 1970’s high socks guy. Always have been and always will be. In terms of a post action de-brief, my only real suggestion is to offer the option of high-top vs ankle socks.
The anesthesiologist came by and said hello and asked if I had any questions. I don’t remember even talking about anesthesia. I wasn’t bothered because I knew I’d never see him again. My nurse anesthetist arrived a few minutes later and I looked her over critically. I decided I was more comfortable with her pushing my propofol, than the anesthesiologist who goofed up with MJ.
Next the Gastroenterology fellow came by to get me to sign my procedure consent. She was an attractive young woman with thick brown hair and an “Ole Miss Rebels” sticker on her ID badge. She told me that about 5 people in a 1000 who have a colonoscopy suffer a serious complication. Perforation of the bowel occurs in about 1 out of a 1000 procedures and the post procedure mortality rate is somewhere between 1 in 3300 and 1 in 330,000. A perforation requires immediate major surgery. Acute and delayed hemorrhage can also occur. Those rates are higher in procedures with a biopsy or polypectomy, and every procedure involves a biopsy or polypectomy.
I probably should have paid more attention. I’ve consented thousands of patients and I’ve talked about these “remote” possibilities each time. As a terrific surgeon, I know they’re never going to happen in my hands. I’m sure my GI fellow believes the same. To be honest, by the time the IV is in, and I’m in my backless gown, you argue that I’m already “all-in.” By the time you’re in the pre-op area, I don’t think you’re supposed to pay attention to the procedural risks.
There was another reason I didn’t pay attention to the details. I couldn’t stop thinking about the fact that this pretty young brunette would be placing a flexible metal endoscope with a fiber optic camera into unbleached private terrain in about 15 minutes. She was very professional and gave no indication of the excitement she felt over the impending festivities.
The GI fellow was followed in by my GI attending. Of course, the first thing he told me was that he’d been one of my medical students many years ago. The first thought that flashed through my head was that I hoped I hadn’t been a jerk. I hoped I hadn’t yelled at him for not knowing how many milliliters of fetal Rh positive blood can be neutralized by an ampule of Rhogam. My attending didn’t let on that he harbored any longstanding grievances that might necessitate a few unneeded abrupt left- or right-handed turns of the colonoscope.
Important teaching point- as a young attending, always remember that one day you will be an old attending and will receive health care from physicians who used to be your students. Behave accordingly. By the way, the answer is 30 ccs of fetal whole blood and 15 ccs of fetal packed red blood cells.
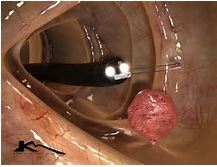
They rolled me into the endoscopy suite at exactly 12 noon which was when my procedure had been scheduled. I wondered why my team wasn’t having lunch, but cheered myself with the thought that they must just love their work. It was a bright shiny room. I glanced quickly at the endoscope to make sure no one had forgotten to drop it into the Cidex sterilizing solution after the last case. It was gleaming and anxious.
My nurse anesthetist asked me to roll on my side and I watched her inject propofol and bubbles into my vein. I was still laying on my side when I woke up in the recovery room about one hour later. I was alert, felt pretty good and felt nothing to suggest that I’d had a bad date.
My GI attending came by moments later to tell me that everything had gone extremely well. I asked him if they’d gotten good imaging and he responded, “You sir, are going on my refrigerator.” I took that as a positive sign. Two small polyps were lassoed, but both were small and appeared completely benign. Pathology is pending.
Which brings me to the last part of my blog. The efficiency, precision, expertise and comfort that the MUSC Gastroenterology Division brings to the colonoscopy procedure is absolutely amazing and something to be envied. However, similar attention now needs to be directed at the prep.
When I had my first colonoscopy, I was in some sort of study and received a handful of pills and a medium-sized glass of Gatorade the night before. It wasn’t too bad, but I was chastised the next day for being “poorly prepped.” Turns out that I’d been in a failed study group. This time I got the full horrible experience.
Sunday, I was supposed to only take clear fluids which was okay because I decided I could see through Mt Dew. Nothing red or purple which brings up questions I don’t particularly want answered. At 6 pm I was to begin drinking a gallon of GraviLyte-N with Flavor packet – one quart each hour. The pharmacist told me how much she personally liked it, especially chilled and with the delicious lemony flavor packet. She is crazed and I’ve already reported to the S.C. Medical Board.
It was nasty stuff and I threw up after the first quart. A Zofran got me through the next 3 quarts. I did not appreciate the irony when I sat down to watch A River Runs Through It on HBO. GaviLyte-N contains 420 grams of “Polyethylene Glycol 3350” and even a delicious flavor pack can’t hold back that raging bull. The 3350 is the number of times I went to the bathroom between 10 pm and 10 am. I was squeaky clean and clear.
If we can send a man to the moon, put chili cheese flavoring on Fritos and take a high resolution guided-tour and photo montage of my large bowel without me even being aware, then we have to be able to come up with a better prep. About 4 am, I was wondering how many people die each year from the colonoscopy bowel prep alone.
Several quick suggestions to make the prep go better:
1. Plan to spend the day at home in comfortable surroundings with ready access to the toilet
2. Better yet, plan to spend the day in a 4 – star hotel with ready access to the toilet (it’ll be its last day as a 4-star hotel)
3. Consider flying to France to a hotel room with a bidet
4. Get the GaviLyte –N as close to freezing as you can
5. Forget the flavor packet. Try the zero calorie flavored water enhancers – 2 squirts per 8-oz glass of GaviLyte slushie
6. Pre-medicate with an anti-emetic (ODT Zofran) and a couple of Tylenol
7. If you try to sleep don’t be ashamed to try-out some adult diapers
8. High quality toilet tissue at the least; Cottonelle cleansing cloths even better
9. A soothing salve such as petroleum jelly for when the situation starts getting dicey
10. Pray for some serious advances in medical science or for guardian angels to come and do the bowel prep for you.
All in all, it is now Tuesday and I’m only very minimally worse for wear. I’m not looking forward to the next one, but other than the prep, I don’t believe it would be possible for the colonoscopy to go any easier. I thank my team for a job very well done and a great experience at the Ashley River Tower Endoscopy Laboratory.
In my limited research for this blog I did find a meta-analysis that found playing music during the procedure increased tolerability. I don’t think it would’ve been possible for me to have been more tolerant. However, it does bring up the question of the appropriate Springsteen music video that I link to every blog. In one song or another Springsteen touches on almost every major life event. The one exception may be colonoscopy. In a reach, I’ve selected the 1992 classic Human Touch.
As a tenured Professor and Maas Chair for Reproductive Sciences I have practiced at MUSC for over 30 years in the Department of Obstetrics and Gynecology. However, the opinions in this blog are mine alone and not those of my employer.

Great recap. Too funny and accurate